Anxiety Disorders (phobias)
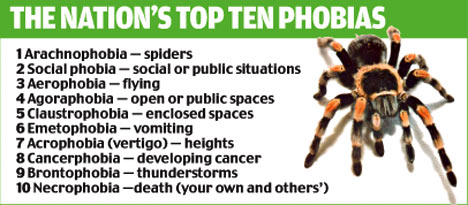
Anxiety disorders are to do with feelings of fear, apprehension and tension that people experience. Everybody experiences anxiety at some time in their life, a threat will cause a person to be fearful and prepare themselves for the ‘flight or fight’ biological response. However, for some people, the level of anxiety experienced is very high and seriously affects their ability to function properly in everyday life. One common example of an anxiety disorder is phobias.
Bullet point 1 - Definitions, Types/examples (case studies) of phobias
definitions, types/examples (case studies) of phobias
Types: e.g. agoraphobia, blood phobia, dog phobia
Types: e.g. agoraphobia, blood phobia, dog phobia
Definition of a phobia
|
A phobia is an extreme and irrational fear of an object or situation, which is disproportionate to the actual danger involved, and leads to avoidance of that object or situation.
A fear becomes a phobia when it begins to be maladaptive, i.e. when it begins to interfere with everyday life. SYMPTOMS The typical symptoms of a phobia are:
|
There are three categories of phobia:
· Specific phobia – an intense and irrational fear of a particular item or situation, such as animals or places. · Social phobia – a persistent and irrational fear of social situations. Of interacting or performing in front of people. · Agoraphobia – a fear of having a panic attack in a public place. Fear of open spaces. |
Types of phobias
Specific phobiaA specific phobia involves a strong fear and avoidance of a particular object or situation. When exposed to the feared object or situation an individual will experience great anxiety, a panic reaction often occurs and the situation or object is usually avoided. Sometimes simply anticipating exposure to the feared object can bring on a panic attack.
In addition to the points above, to be diagnosed with a specific phobia the fear must:
Specific phobias are quite common, affecting 10% of the population, and are more prevalent in women than in men. Fear of dogs might be one common example. Fear of blood is different from other specific phobias as the person may actually faint at the sight of blood and may therefore avoid seeking medical attention. |
Social phobiaFear of social situations. The high levels of anxiety or panic can result in the person performing poorly in front of others. In an interview situation, for example, the person may perform so poorly that they are not offered the job.
People with social phobias are often very able, but do not demonstrate this in front of others because the anxiety is so debilitating. Often the anxiety is so strong that it causes avoidance of certain situations altogether. When the social anxiety interferes with work and social life it becomes a clinical condition. Generally people with social phobia feel inadequate in comparison to other people and find relationships difficult. To compensate they may become workaholics or develop all-consuming hobbies. Social phobias occur more in women than men often starting during adolescence and seem to be more common in families where parents and relatives use shame as a way of controlling a child’s behaviour. Social phobias are NOT just "shyness", they are far more. |
AgoraphobiaAgoraphobia is a particular fear of open spaces. Approximately 2-3% of the population suffer from agoraphobia and the majority are women.
Research has shown that agoraphobia develops as a result of severe panic attacks that the person does not expect to happen (Barlow 2002). There are two types of agoraphobia: 1. Agoraphobia as a complication of panic attacks. Agoraphobics are anxious about having a panic attack in a public place and being unable to escape or find help. The person then engages in avoidance behaviour, which results in staying at home, not going outside and becoming fearful at the simple thought of going out. 2. Agoraphobia without panic attacks. This is less common than the above type, and is characterised by a spreading fear of the environment outside the safety of the individual’s own home. This fear gradually increases in severity, until eventually the person can become housebound. |
|
Assignment 1 - Test your diagnosis
Assignment 2 - Section A questiona) Define what is meant by the term 'phobia' (2)
b) Describe two different types of phobia (4) | ||
Examples of phobias
Below are a couple of case studies of people with phobias. In both cases, you can start to see some possible treatment methods for the phobias too... Make sure you can pick out the features of these cases which make them a phobia (rather than just a fear). How do they match the criteria given above?
|
|
|
Bullet point 2 - Explanations of phobias
• explanations of phobias
Behavioural (classical conditioning, e.g. Watson, 1920); Psychoanalytic (Freud, 1909); biomedical/genetic (e.g. Ost, 1992); cognitive (e.g. DiNardo et al., 1988)
Behavioural (classical conditioning, e.g. Watson, 1920); Psychoanalytic (Freud, 1909); biomedical/genetic (e.g. Ost, 1992); cognitive (e.g. DiNardo et al., 1988)
Behaviourist explanations of phobias
|
First download and complete the document below, which helps you to remember the key features of behaviourist theory. You should be an expert on this by now!
BUT... can you see how behaviourists would explain the formation of a phobia? Phobia fits very nicely into behaviourist theory. See if you can predict this before you read on. Assignment 3 - behaviourist phobias
|
| ||

|
You should be able to remember the theory of classical conditioning from the AS section on Behaviourism. If you can't, review it here.
Then, try to analyse the Little Albert experiment in the video above, including the following terms: "unconditioned stimulus, conditioned stimulus, neutral stimulus, unconditioned response, conditioned response" |

|
Maintaining phobias - Avoidance conditioning
|
Classical conditioning works well for explaining how phobias might be formed, but not why they might be maintained. The two-process
theory (or two-factor theory) by Mowrer (1947) involves both classical and
operant conditioning and is generally known as avoidance conditioning.
It suggests that the fear develops through classical conditioning – we learn to associate an object or situation with being frightened. This fear is then maintained by operant conditioning because the person learns that their fear is reduced by avoiding the stimulus. People will avoid contact with mice and therefore do not get the fearful response – negative reinforcement. For example, Little Albert would be classically conditioned to fear the rat and this would be maintained by operant conditioning – by avoiding rats, which would reduce his fear response and strengthen his fear of them, making him want to avoid a rat in the future. |
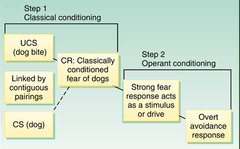
The two process theory. Classical and operant conditioning working together to form and them maintain a phobia.
|
Social learning theory and phobias

|
Remember SLT from Bandura's experiment...? Recap here if not
Phobias could develop as a result of watching/observing another person (the model) experience the pain/upset from an object/situation. If the observer is a young child, the model may be the mother or father. Example: if a mother has a fear of spiders and reacts in a highly emotional and extreme way when there is a large spider in the bath, the child may also develop a phobia for spiders. This is because the mother acts as a role model for the child, and because the strong emotions of the mother towards the spider may frighten the young child. Here, classical conditioning would operate to pair the spider with the fear reaction of the mother, resulting in fear of spiders in the young child. |
Evaluation of behaviourist explanations of phobias
|
Look at this great flow chart of behaviourist explanations and treatments from Aiden Sammons!
|
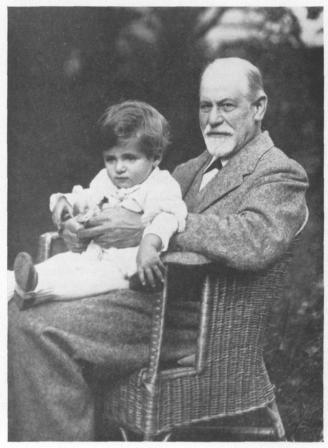
The Psychoanalytic explanation of phobias
Just like the behaviourist explanation, you've done this before. Remember Little Hans? This is the most famous case of a phobia which was explained using Freud's approach, so you're already a bit of an expert!
Freud's theory is based on the idea that people have unconscious wishes and thoughts that cause unconscious conflict between the ego and the id or superego. The ego is threatened by unconscious conflict and fears that the anxiety caused by the conflicts will overwhelm it. Because the entire ego’s energy is being used trying to cope with the anxiety or feelings of panic the ego may not be able to function at all.
To cope with this, the ego uses the defence mechanism DISPLACEMENT – the anxiety is displaced onto another object or situation. This results in a specific phobia, it is less threatening to the individual to have a phobia than it is to have the unconscious thoughts and conflicts without trying to do anything about them. Either way the person is trapped in a no-win situation since the phobia can be as debilitating as the original unconscious thoughts and desires.
Freud's theory is based on the idea that people have unconscious wishes and thoughts that cause unconscious conflict between the ego and the id or superego. The ego is threatened by unconscious conflict and fears that the anxiety caused by the conflicts will overwhelm it. Because the entire ego’s energy is being used trying to cope with the anxiety or feelings of panic the ego may not be able to function at all.
To cope with this, the ego uses the defence mechanism DISPLACEMENT – the anxiety is displaced onto another object or situation. This results in a specific phobia, it is less threatening to the individual to have a phobia than it is to have the unconscious thoughts and conflicts without trying to do anything about them. Either way the person is trapped in a no-win situation since the phobia can be as debilitating as the original unconscious thoughts and desires.
Assignment 4 - Remembering Little HansLook back at the study of Little Hans. How does this case fit with the theory described above? Write a short summary of Hans' phobia from Freud's perspective. How is displacement occuring? What are the unconscious thoughts causing anxiety? What symbols are created by the sufferer?
Other phobias from a psychodynamic perspectiveIn similar fashion to Freud other Psychodynamic theorists have argued that a fear of spiders hides unconscious conflicts. For example, according to Sperling (1971) a fear of spiders is a defence against more threatening impulses of a sexual nature. Abraham (1927) proposed that the fear of spiders is symbolic of an unconscious fear of sexual genitalia.
The psychodynamic approach explains agoraphobia as resulting from separation anxiety experienced by a young child. This is at the unconscious level and is to do with irrational thoughts that the child has about being separated from the mother and the realisation of dependency on the caregivers. Agoraphobia serves the function of keeping the person at home, and for the unconscious, irrational mind this reduced separation anxiety. This is because, unconsciously, the person thinks that separation from either or both parents is less likely if the person is at home all the time. |
|
Evaluating psychodynamic treatments of phobias
Assignment 5 - how would you explain these phobiasYou are Sigmund Freud. How would you use psychodynamic theory to explain the phobias in the document below?
|
|
| ||
Biomedical/Genetic explanations for phobias
Some people seem more susceptible to developing a phobia than others, and therefore a genetic explanation has been proposed to account for these individual differences.
Before you read any further, ASK YOURSELF "What sorts of methods would be used to investigate the genetic basis of phobias?" Based on what you already know from other biological and genetic explanations, you should be able to suggest this in detail already...
Before you read any further, ASK YOURSELF "What sorts of methods would be used to investigate the genetic basis of phobias?" Based on what you already know from other biological and genetic explanations, you should be able to suggest this in detail already...
Some initial biological evidence - Ost (1992)J Abnorm Psychol. 1992 Feb;101(1):68-74.
Blood and injection phobia: background and cognitive, physiological, and behavioral variables.Ost LG. Author information Abstract: Blood-phobic (n = 81) and injection-phobic (n = 59) patients fulfilling the DSM-III-R criteria for simple phobia were compared on a number of variables. There were no differences between the samples in age at onset, age at treatment, marital and occupational status, history of fainting in the phobic situation, and impairment. Higher proportions of blood-phobic subjects than of injection-phobic subjects reported having first-degree relatives with the same phobia (61% vs. 29%) and reported fearing that they were going to faint in the phobic situation (77% vs. 48%). In both samples, these proportions were higher in the subgroup with a history of fainting. Overall 62% of people with a blood and injection phobia reported a 1st-degree relative who shares the same disorder. The prevalence rate for the general population is just 3%. Injection-phobic subjects rated 2 of 11 physiological items higher than did blood-phobics subjects, but the groups did not differ on behavioral variables. Overall, the similarities were more marked than the differences, and it is suggested that these two specific phobias should be regarded as one diagnostic entity. |

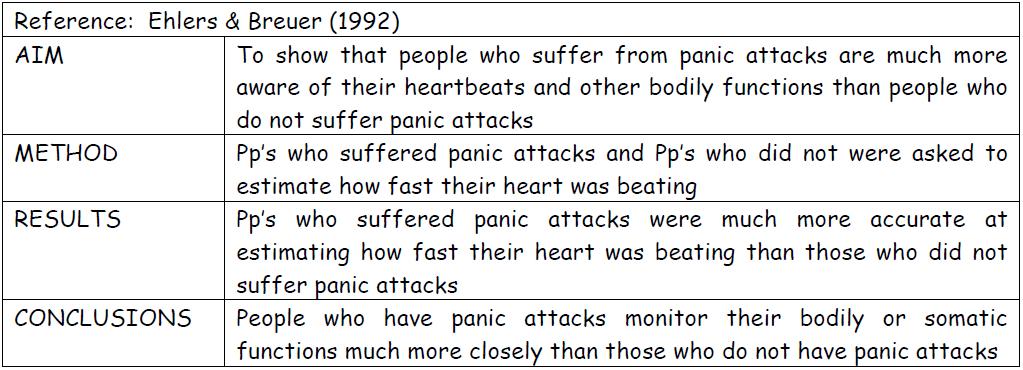
Ost (1992) investigated blood and needle phobias
Assignment 6 - summarising researchRead the abstract of the paper by Ost (1992), and produce a summary of the main findings. Then write three conclusions that could be drawn from the research, and three evaluations of it.
|

'Preparedness' might explain why we see this harmless bit of rope as a snake...
|
How does the biological explanation work? - PreparednessThe 'preparedness explanation suggests that human beings have a genetic predisposition to develop phobias to certain items and situations, such as fear of darkness, heights open spaces and strangers. These were potential sources of danger to us thousands of years ago. Those individuals who developed such phobias would avoid harmful objects or situations and would be favoured by evolution.
Seligman (1971) suggested that there was a ‘preparedness’ (a physiological predisposition) to be sensitive to certain stimuli. It is not the fears themselves that are inborn, rather there is an innate (in-born) tendency to rapidly acquire a phobia to potentially harmful events – we are biologically prepared from birth. |
Preparedness - a happy marriage of behaviourism and bio!Preparedness can be explained equally well from a biological and behaviourist perspectives:
Biological – a readiness to fear certain things could have evolved and then been passed on genetically Behaviourist – experience with certain animals, such as snakes or spiders, might have taught us to fear them and in some cases develop a phobia. On other words, we are genetically programmed to develop classically conditioned phobias more rapidly to certain objects! EXAM TIP: In the examination you can discuss this theory under either approach! Two for the price of one! |
It's common to use different approaches as though they are rivals - but that doesn't always have to be the case. They can work well together too!
|
Evidence for preparedness - Ohman et al (1975)AIM Conducted a series of studies to investigate the preparedness explanation of phobia acquisition
METHOD Participants were shown pictures of houses, snakes, spiders and faces of people. Half the participants received an electric shock whenever they were presented with a picture of a house or a face. The other half received an electric shock whenever they were presented with a picture of a snake or spider. RESULTS Both groups of Pp’s showed fear when subsequently shown pictures they had experienced with an electric shock. This was measured by their skin reaction called galvanic skin response (GSR). Following a period in which Pp’s received no electric shocks it was found that the GSR was higher for those shocked when shown snakes and spiders. CONCLUSION Human beings may be more biologically prepared or ready to develop phobias for animals such as snakes and spiders, which may threaten survival. |
Evaluating biological explanations for phobias
|
GENETIC STUDIES:
PREPAREDNESS:
|

Could you have predicted these criticisms? The same issues come up time and time again! The better you understand this, the better you'll do in an exam!
|
Cognitive explanations for phobiasAs you know, in cognitive explanations the fearful response is experienced due to the interpretation or appraisal of events. It is the interpretation of an event that triggers the emotion not the event itself.
When a person has a phobia, their response to a situation/object is immediate and extreme, and the interpretation and appraisal distorted. Phobias form and persist due to three main factors: |
|
|
Irrational or negative thought processesNegative self-talk/negative images – these include 3 basic distortions:
|
Example of a case study for cognitive explanations - agoraphobia
According to cognitive theory, the agoraphobic person is hypersensitive to spatial layouts in the environment and also to being too far away from a someone who could take care of them. If access to home or the caretaker is blocked then fear is induced and the agoraphobic has an urgent need to return home. They may catastrophise what can happen in open or crowded spaces (e.g. "what if one of these people attacks me?"), or over-estimate the danger they are in ("there's nowhere here that's safe"). As a result of this, the person might begin to avoid open spaces, becoming house-bound and rarely going outside.
Beck et al (1985) proposes that agoraphobics possess latent fears of situations that might have been potentially dangerous to a child but are not dangerous to
adults, for example, crowded shops or open spaces. This explains the sensitisation.
Beck et al (1985) proposes that agoraphobics possess latent fears of situations that might have been potentially dangerous to a child but are not dangerous to
adults, for example, crowded shops or open spaces. This explains the sensitisation.
Here is another study which nicely illustrates the idea of cognitive vulnerability
|
Research supporting the cognitive approach - Di Nardo et al (1988)DiNardo et al. (1988) reported that 56% of dog phobics had an unpleasant encounter but about 50% of normal controls had also had such experiences and did not develop a phobia. Behaviourism ignores cognitive factors and so cannot account for individual variation. The fact that not all phobics have had a bad experience and some non-phobics have had a bad experience and not developed phobia is probably due to the patients’ perception and interpretation, and so cognitive rather than behavioural factors are important.
|
Evaluation of cognitive explanations of phobias
- They accept the acquisition of fear through learning, for example, conditioning, but also emphasis the person’s own interpretation of events. They therefore present a more holistic explanation than some others.
- The cognitive explanation is a coherent theory with practical therapeutic applications. The treatments have proved highly effective for anxiety disorders such as phobias. The success of the treatments supports the explanation.
- Psychologists can conduct experiments to identify the different though processes of those who have a phobia and those who do not. This makes the explanation scientific and objective.
- BUT behaviour is not always driven by cognitions, evidence suggests that cognitions can be driven and/or maintained by inappropriate behaviour such as avoidance. Therefore behaviourist ideas may sometimes be more effective for explaining a phobia.
Bullet point 3 - Treating phobias
• treating phobias
Systematic desensitisation (Wolpe, 1958); flooding; applied tension (Ost et al., 1989); cognitive-behaviour therapy (Ost and Westling, 1995)
Systematic desensitisation (Wolpe, 1958); flooding; applied tension (Ost et al., 1989); cognitive-behaviour therapy (Ost and Westling, 1995)
Two types of behaviourist treatments for phobias
Remember that behaviourists would explain phobias as a learned association between a certain stimulus (e.g. dogs) and a certain response (e.g. fear). Behaviourist therapies will therefore try to reduce the strength of these associations. There are two main methods used to try to do this
Systematic desensitisationThis involves the gradual exposure of the sufferer to the phobic object.
Developed by Wolpe (1958) it is based on the idea that two emotions cannot occur at the same time. There are 2 key aspects to this technique: • Getting people to practise relaxation techniques when feelings of tension and anxiety arise • A stepped approach to getting the person to face the object or situation of their phobia (a hierarchy). e.g. The top of the hierarchy might be touching the phobic object, whereas the bottom of the hierarchy might be having one in the same room. Slowly, the object can be moved through the hierarchy until the fear can be replaced with relaxation. The video below shows this happening very clearly, as does this one. 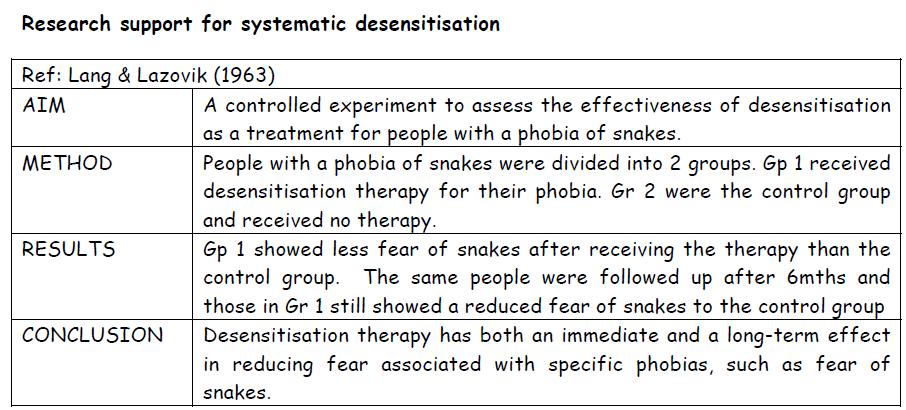
Virtual reality exposure therapy (VRET)
This is a new technique based on the principles of systematic desensitisation, but the therapy takes place in a virtual world. Although used largely to date with phobic patients, it is being trialled with other anxiety disorders too.
Patients are placed in a 3-dimensional virtual world where they wear a head mounted display which allows the individual to pick up sensory cues. A computer monitor shows the therapist what the patient sees. This video shows it in action for arachnophobia |
FloodingThis involves a sudden, overweening exposure to the phobic object; overwhelming the individual’s senses with the item or situation that causes anxiety so that the person realises that no harm will occur and in fact there is no objective basis for their fear.
The steps that are involved in this are: 1. A patient is exposed to the object/situation that causes anxiety (e.g. a room full of snakes) 2. The patient is initially overwhelmed and very fearful, but this subsides after a while 3. The patient recognises that anxiety levels have dropped and that although such situations have been avoided in the past, there is in fact no reason for this. The video above shows this process: 
|
Evaluating behavioural therapies for phobias
- Systematic desensitisation is supported by empirical evidence, which shows it often be an effective treatment for specific phobias (e.g. Lang and Lazovik).
- Systematic desensitisation works well in the therapeutic situation and is a quick and cost effective method. However the therapeutic effect does not always generalise to the patient’s everyday life (as real life is not as controlled as the therapy).
- On vivo (real-life exposure) is more effective that in vitro (imagined exposure) for both flooding and systematic desensitisation.
- VRET has advantages over systematic desensitisation as it is much easier and cheaper and often more convenient, but still has a similar level of success.
- The equipment required for VRET is expensive and may not be suitable for all phobias. In addition patients do sometimes report negative side-effects e.g. nausea
- Systematic desensitisation can only be used when a particular phobic object/situation can be identified. It is suitable for phobias of snakes/spiders etc but not for generalised social phobias, so it is only useful for certain cases.
- Flooding produces high levels of fear and this can be very traumatic, and therefore has ethical implications.
Applied-tension therapy for phobias
The Applied Tension Technique is a strategy developed to help prevent fainting or help people recover faster if they do faint. It is specifically useful for phobias associated with fainting, usually needle and blood therapies.
The technique involves tensing the muscles in your body, which then raises your blood pressure. If your blood pressure increases, you are less likely to faint. Participants are taught to tense their major muscle groups at the first sign of faintness.
The technique involves tensing the muscles in your body, which then raises your blood pressure. If your blood pressure increases, you are less likely to faint. Participants are taught to tense their major muscle groups at the first sign of faintness.
Ost et al (1989)Abstract: Thirty patients with phobia for blood, wounds and injuries were treated individually with applied tension, applied relaxation, or the combination of these two methods for 5, 9 and 10 sessions. respectively. They were assessed on self-report, behavioural and physiological measures before and after treatment, and at a 6-month follow-up. All groups improved significantly on 11 12 measures, and the improvements were maintained at follow-up. Applying stringent criteria, 73% of the patients were clinically improved at the end of treatment and 77% were so at follow-up. Despite a failure to find between-group differences, on many measures there was a trend favouring applied tension. Since this method is as effective as the other treatments in only half the time, applied tension should clinically be the treatment of choice for blood phobia.
Assignment 7 - Summarising researchWrite three conclusions and three evaluations of the study described above.
|

Applied tension - tensing various muscle groups to raise blood pressure and prevent fainting.
|
Applied tension - how to do it
TIP: When you relax your muscles after tensing them, the goal is not to become completely relaxed, as this will cause your blood pressure to drop. Rather, the goal is to let you body return to a normal state (not overly tense or completely relaxed). It is important that you practise this strategy several times a day for at least a week. |
Evaluating applied tension theory
|
Cognitive-behaviour therapy for phobias
|
You know by know that the aim of cognitive therapy will be to replace unrealistic and fearful thinking about phobias with more realistic mental habits. It teaches patients to identify, challenge and replace counter-productive thoughts with more constructive thinking patterns. The task is to get the client to see that their thoughts are irrational and not based in reality.
|
Remember RET?You should remember Ellis' RET (1970) from the abnormal affect page. It can also be used to treat phobias! The client tells the therapist exactly what unrealistic, distorted and catastrophic thoughts they have. The therapist helps the client change these thoughts to ones that are rational andmore normal ways of thinking.
|
Cognitive rehearsalCognitive rehearsal helps the individual to think about and mentally rehearse appropriate behaviours, so that when it comes to the real thing these behaviours can be enacted. It helps to stop the person thinking about the negatives.
For example, in social phobia a client is asked to think about specific behaviours that are appropriate to the social situation, they then rehearse the appropriate behaviours to perform. For example clearly introducing themselves and saying what the topic of the presentation is, referring to notes when the different slides come up, looking at the audience and asking if anyone has any questions at the end of the presentation. When it comes to the actual presentation the client enacts these behaviours. Challenging distorted thinking often also involves using counterstatements.
Using Counterstatements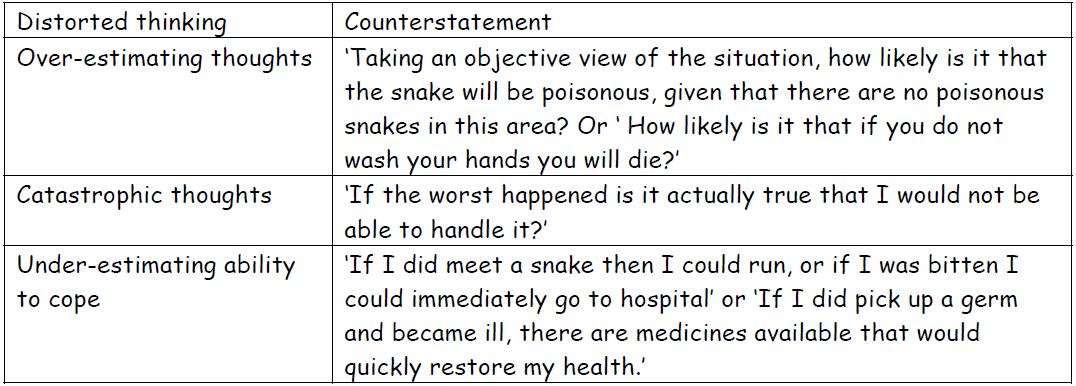
Examples of counterstatements for some of the common cognitive distortions associated with phobias. Click to enlarge.
|
Key study - Ost and Westling (1995)
Assignment 7Write half a page from memory summarising each treatment option listed in this section
|
Aim - To compare cognitive behaviour therapy (CBT) with applied relaxation as therapies for panic disorder.
Method - A longitudinal study with patients undergoing therapy for panic disorder. Design - Independent measures design with patients being randomly assigned to either applied relaxation or CBT. Participants - 38 patients with DSM diagnosis of panic disorder, with or without agoraphobia. Recruited through referrals from psychiatrists and newspaper advertisements. 26 females and 12 males, mean age 32.6 years (range 23–45 years). From a variety of occupations and some married, some single and some divorced. Procedure - Pre-treatment: baseline assessments of panic attacks, using a variety of questionnaires (e.g. the Panic Attack Scale, Agoraphobic Cognitions Questionnaire, etc.). Patients recorded details of every panic attack in a diary. Each patient was then given 12 weeks of treatment (50–60 minutes per week), with homework to carry out between appointments. Findings - Applied relaxation showed 65% panic-free patients after the treatment, 82% panic-free after one year. CBT showed 74% panic-free patients after the treatment and 89% panic-free after a year. These differences were not significant. Complications such as generalised anxiety and depression were also reduced to within the normal range after one year. Conclusion - Both CBT and applied relaxation worked at reducing panic attacks, but it is difficult to rule out some cognitive changes in the applied relaxation group even though this is not focused on in this research. |
Evaluating cognitive therapies - YOU'VE SEEN THESE BEFORE!!!
|
|
End of section essay writing exercise - Section B
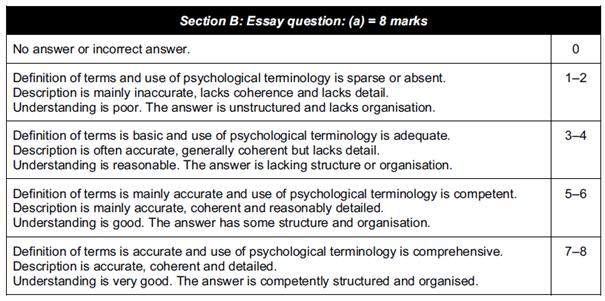
14 (a) Describe what psychologists have discovered about phobias. [8]
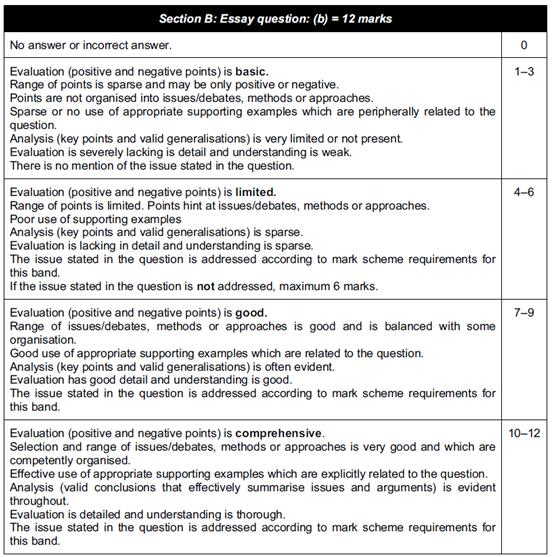
(b) Some psychologists argue that phobias are learned just like any other behaviour. Evaluate what psychologists have discovered about phobias and include a discussion of the behaviourist explanation of phobias. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it the behaviourist explanation. At least a paragraph should consequently be devoted to discussing the behaviourist approach.
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.
(b) Some psychologists argue that phobias are learned just like any other behaviour. Evaluate what psychologists have discovered about phobias and include a discussion of the behaviourist explanation of phobias. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it the behaviourist explanation. At least a paragraph should consequently be devoted to discussing the behaviourist approach.
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.

|
|
End of section essay writing exercise - Introducing Section C
Section C in your exam always consists of two questions, one 6 mark recall question and one 8 mark application question. There are always two of these types of question, and you need to choose one.
You are a practising psychotherapist and you know how to treat patients and the underlying causes of disorders. One of your patients is a male who has a fear of women.
15 a) Describe the main features of psychotherapy. [6]
15 b) Suggest how you would use psychotherapy to help your patient to resolve his fear of women. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here you have to suggest how you would use psychotherapy to treat the patient. You therefore need to make sure that you are specifically referring to ideas of psychotherapy, and to the condition given in the question. It takes some getting used to writing this way, but it is an area that, with a little bit of practice, you will be able to do very well on.
Have a go at the questions above. Please submit your essays through the form on the home page.
You are a practising psychotherapist and you know how to treat patients and the underlying causes of disorders. One of your patients is a male who has a fear of women.
15 a) Describe the main features of psychotherapy. [6]
15 b) Suggest how you would use psychotherapy to help your patient to resolve his fear of women. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here you have to suggest how you would use psychotherapy to treat the patient. You therefore need to make sure that you are specifically referring to ideas of psychotherapy, and to the condition given in the question. It takes some getting used to writing this way, but it is an area that, with a little bit of practice, you will be able to do very well on.
Have a go at the questions above. Please submit your essays through the form on the home page.
Revision |
Extension |
