Abnormal Affect
Disorders of affect (emotion) are probably the most common form of psychological disturbance. Whereas it can be hard for us to understand and imagine the symptoms of schizophrenia, we are all familiar with the symptoms of depression, and we all have had some experience of 'low mood' at many points in our lives. However, it is perhaps precisely because it seems more familiar, that people with major depression still feel misunderstood, as we often feel that people should be able to 'snap out of it' like we might do with a bad mood. For the 15% of people who it is estimated will have a major depressive episode at some point in their lives, this is not a condition that can be easily shaken off...
Bullet point 1 - Types, Characteristics and examples of Sex Differences
types, characteristics, examples of and sex differences
Types: depression (unipolar) and mania (bipolar); causes and treatments for manic depression; sex differences in depression
Types: depression (unipolar) and mania (bipolar); causes and treatments for manic depression; sex differences in depression
Types of abnormal affect conditionsDepression is the main symptom of a number of mood disorders, which include the following.
Major depression (Unipolar) Manic depression (bi-polar) Seasonal affective disorder (SAD) Far less studied and seemingly much rarer is the opposite of depression... unipolar mania! 
|
Bipolar depression (or manic depression)Bipolar disorder is characterised by alternating periods of depression and mania (high mood); which seem to be unrelated to an external event. The length of time and the frequency vary from person to person. The manic and depressive episodes can be separated by long periods of normal functioning or the episodes quickly follow one another. During the manic phase the person may lose touch with reality and the illness is therefore categorised as a psychosis
Diagnosis of bipolar depression In the depressed phase the symptoms are very similar to those in Unipolar disorder (see below), however there are additional symptoms in the manic phase. Cognitive – thought processes may be disturbed to the extent hast they have delusional ideas i.e. believing they are a famous person. They may also make irrational and reckless decisions. Emotional – they will feel fantastic! They obviously tend to deny that there is anything wrong with them. There is also a lack of social inhibitions because of their new found confidence. Behavioural – they tend to talk faster and may become reckless with negative consequences. Physical – during this phase the person will have very little sleep and have an increase in energy levels, becoming much more active than normal. More males than females tend to be diagnosed. Age of onset is usually early 20s. The symptoms for both mood states must have been experienced for a diagnosis to be made. They may be admitted without consent because during the manic phase they may deny anything is wrong with them and so appear to suffer from psychosis. |
Causes of bipolar disorderSTUDY – Price (1968) - Genetic evidence for bipolar depression
AIM: Price wanted to provide evidence of a genetic cause in bipolar disorder by looking at the concordance rates for bipolar MZ and DZ twins METHOD: he looked at sets of identical (MZ) and non-identical (DZ) twins. It was expected that identical twins would have similar psychological functioning as they share 100% of their genes. Whereas the concordance rate for bipolar in DZ twins should be much less as they only share 50% of their genes. RESULTS: Concordance rates:
CONCLUSION: the results are strong evidence for the role of genetics; the more closely related MZs have a far greater concordance rate. The most revealing factor was that the concordance rate for twins was almost the same for those reared together and those reared apart - therefore implying that nurture is far less important than nature (genes). ADOPTION STUDIES also provide genetic evidence. A study by Cadoret (1978) looked at 126 adopted children, 8 of which were born to a parent with manic-depression, but adopted by a healthy couple neither of whom suffered from depression. Three of those 8 later developed a major affective disorder, compared to only 8 of the remaining 118 children. Stephen Fry is a British TV personality who has spoken movingly about his fight with bipolar disorder and has made some excellent programs on it. Part 1 of his documentary 'The Secret Life of The Manic Depressive' is on the right. |
Treatments for bipolar disorderDrug treatment for the manic phase of bipolar disorder has lagged behind that for major depression.
|
Exam success tip! Drawing links between units when evaluating genetic evidence
The Price (1968) study given above presents genetic evidence for bipolar disorder, using a twin study methodology. We have already looked at twin and family studies in the first two sections, and you should already be familiar with the major criticisms of them. If not, go back and look at them again. It is crucial that you can draw links and use ideas from different units across the whole course if you are to succeed in your exam.
How would you evaluate the evidence presented by Price? Write half a page evaluating the findings and their implications. Assignment 1Write half a page from memory for each of the following questions.
|
Sex differences in depressionIn adults, major depressive disorder affects twice as many women as men. For both genders it is most common in those who are 25-65 years of age, and least common for those over the age of 65. In children, clinical depression affects girls and boys at about the same rate.
What is not clear is whether this sex difference is due to nature or nurture factors. For example, a nurture explanation could be that females typically have more stressful lives in many countries (due to inequalities between genders, a lack of social status and so on) and this may contribute to higher levels of depression. A nurture explanation would suggest that some biological difference between men and women (perhaps due to genetic or hormonal factors) affects the likelihood of acquiring the condition. 
|
Unipolar depression (major depression)
Unipolar depression is the term used when a person’s mood changes from normal to depressed. People suffering from this type of depression are usually aware their mood has changed and will seek help or make a spontaneous recovery. Unipolar depression can be divided into two different types:
1) Reactive – caused by factors external to the person such as stressful life events, bereavement, divorce etc. This is the type that people are most likely to experience.
2) Endogenous – caused by factors within the person such as genes or brain chemistry
1) Reactive – caused by factors external to the person such as stressful life events, bereavement, divorce etc. This is the type that people are most likely to experience.
2) Endogenous – caused by factors within the person such as genes or brain chemistry
Diagnosis of Unipolar depressionMay appear gradually or suddenly and it occurs in all social classes and all ages. Severe forms mostly occur in middle and old age. In the UK more women than men are diagnosed. But the male suicide rate is much higher than the female rate.
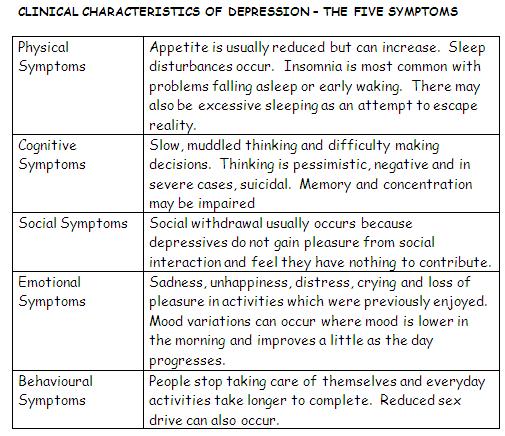
Depression can be diagnosed through clinical interview and use of DSM-IV and ICD-10, which are manuals used in the clinical diagnosis of psychological/psychiatric disorders. There are several factors that the clinician must take into consideration: · Five of the physical, emotional, cognitive, behavioural and social symptoms to occur along with persistent low mood for a minimum of two weeks
|
|
Difficulties in diagnosing depression· Many of the symptoms reported by those suffering mental illness are very subjective (e.g. I feel depressed) – reliant on self-report by the client.
· The reliability of diagnosis may be questionable as DSM-IV and ICD-10 are based on the assumption that we can assign individuals neatly into categories. However, many of the symptoms of depression for example, are found in much of the population. · There may be cultural, social and gender biases in diagnosing people according to classification systems which are devised by western practitioners. Notions of abnormality vary across groups and time. |
Implications/Consequences of being diagnosed with depression
· Once a person has been classified as having a mood disorder a suitable treatment can be decided upon. Patients therefore get access to specialist help.
· A diagnosis of mood disorder can lead to labelling. The stigma of a psychiatric diagnosis may create expectations in the person and others. · There are also issued to be considered concerning the person’s safety. Doctor’s need to assess whether the person is at risk of suicide and if they feel they are, they would need to section them under the mental health act. In turn, this leads to ethical issues pertaining to consent and enforcing treatment. |
STOP and think like a psychologist! You've seen these issues before!!The difficulties and implications with diagnosing depression are often the same as with diagnosing any psychological condition! You can reuse the same ideas to answer different questions, as long as you adjust the point you're making to the specific question being asked.
|

|
|
|
Assignment 2Half a page from memory:
Outline two issues which may arise when diagnosing abnormal affect or any other psychological disorder (6) Assignment 3 - Section A questions(a) Explain, in your own words, what is meant by the term ‘abnormal affect’. [2]
(b) Describe two types of abnormal affect. [4] |
Bullet point 2 - Explanations of Depression
• explanations of depression
Biological: genetic and neurochemical; cognitive: Beck’s cognitive theory; learned helplessness/attributional style (Seligman, 1979)
Biological: genetic and neurochemical; cognitive: Beck’s cognitive theory; learned helplessness/attributional style (Seligman, 1979)
Biological explanations of depression - genetic
Assignment 4 - interpreting research evidence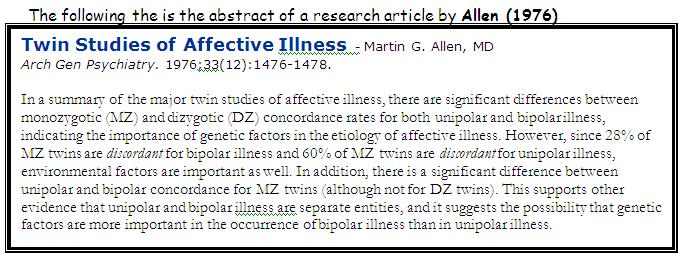
click to enlarge
Above is the abstract of a research article into the genetics of depression. Summarise what you think these findings show (in your own words) and bring them to the next lesson.
|
McGuffin et al (1996)
AIM – To examine the impact of genes on unipolar depression.
METHOD – 177 people with unipolar depression and twins of the same sex were recruited. RESULTS – Concordance rate of 46% for 68 pairs of MZ twins. For 109 pairs of DZ twins it was 20%. Assignment 5 - You draw the conclusionWhat conclusions can you draw from the above study. Make the inferences you draw as detailed as possible and try to consider both what the data shows and what it doesn't show! Write your conclusions down and send them to me.
|
You already know the strengths and weaknesses of genetic explanations (and of the twin studies that they use)! We covered them in schizophrenia, and they're the same here! Learn them once, and you'll be able to use the same points for every genetic explanation!
|
|
Biochemical explanations for depression
You should remember from the models and schizophrenia pages, that the brain produces chemicals to pass messages between different parts of the brain and nervous systems. The chemicals are known as neurotransmitters (as they transmit messages between neurons). The biochemical explanation for depression argues that depression involves the neurotransmitters serotonin and norepinephrine, both of which play a role in appetite and emotion. Lower levels of these chemicals may lead to depression.
Study - Teuting (1981)AIM: to investigate any abnormalities in the urine samples of depressed persons
METHOD: when norepinephrine and serotonin are broken down by enzymes, a chemical compound is present in the person’s urine. Teuting compared the urine samples from depressed and non-depressed people. RESULTS: There were lower levels of the chemical compound in the depressed samples urine in comparison to the non-depressed group. CONCLUSION: this suggests that depressed people have lower than normal activity of NTs in the brain which causes the depressed mood. EVALUATION: difficult to establish cause and effect. Evaluation of biochemical explanations for depression· Anti-depressants do not work for all patients. Also, the drugs increase the levels of the biochemicals immediately but can take weeks for the depression to be alleviated. Why is this? This seems to challenge a direct link between NTs and depression.
· Cause, effect or correlation? It is difficult to establish whether the low levels of NTs cause depression, are an effect of having the disorder or are merely associated with it. Causation cannot be inferred as only associations have been identified. |
Other evidence supporting a biochemical explanation for depression· The 2 neurotransmitters that are thought to be involved in depression, norepinephrine and seratonin, are part of the ‘monoamine group’ that play a role in normal arousal and emotion. That these NTs would be involved in depression therefore seems to have face validity.
· Anti-depressant drugs (MAOIs) which increase levels of norepinephrineand serotonin are often successful at reducing the symptoms of depression as do SRRIs which inhibit the re-uptake of serotonin. 
|
Assignment 6 - Section A question
a) Explain, in your own words, what is meant by a biological explanation of depression. [2]
(b) Describe a study investigating the biological explanation of abnormal affect. [4]
(b) Describe a study investigating the biological explanation of abnormal affect. [4]
Beck's cognitive theory of depression
Beck's cognitive triad
|
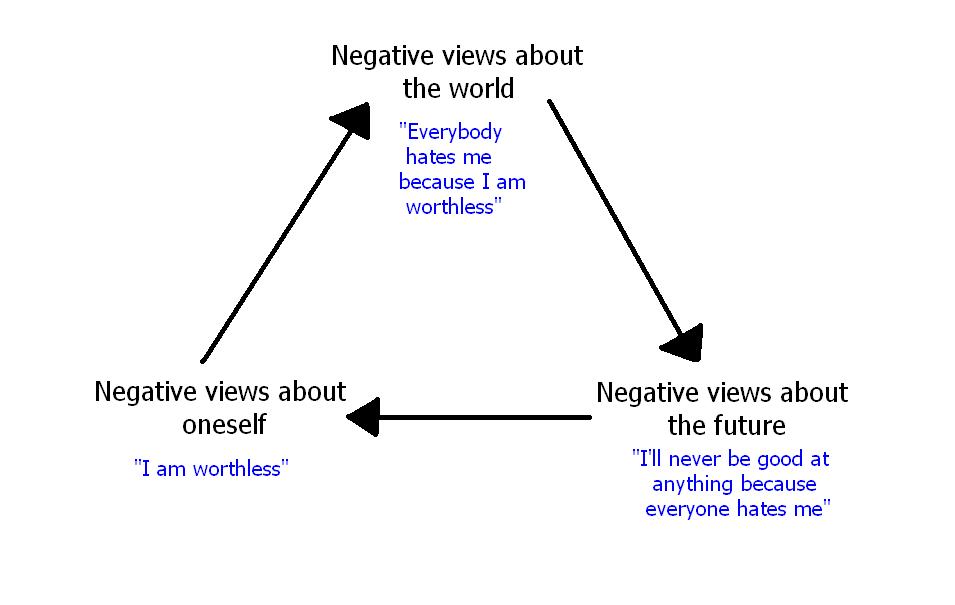
Beck (1987) proposed that people with depression develop negative schemas; they tend to view the world and the future in pessimistic ways. These can become self fulfilling prophesies. Beck (1991) maintains that there are three components to depression:
He called these the cognitive triad. Thus the person sees him/herself as: 1. Worthless 2. Living in a world full of obstacles 3. Contemplating a future continuing in much the same way. The cognitive triad can lead to errors in judgement known as ‘cognitive errors’ such as magnification, minimisation and personalisation, underemphasising strengths and exaggerating weaknesses. |
Evaluating cognitive theories of depression
|
· Cognitive treatments have been found to be as successful as antidepressants supporting the role of cognitive factors in depression
|
· Research is inconsistent so we cannot be sure if negative emotions are a cause or consequence of depression. Maybe depression leads to negative schemas, not the other way around... so there is an issue of the direction of causality here.
· … Lewinsohn et al (1981) found that negative thinking did not precede depression. They concluded that people who had depression were not more likely to have negative cognitions so the direction of causality may be that depression causes negative thinking rather than vice versa… · …There may in fact be a two-way relationship between the two in that negative thinking predisposes depression, and depression increases negative thinking. · Cognitive explanations are less successful for the manic phase in bipolar disorder. |
REVISION - Quizlet on cognitive explanations for depressionHave a go at this quizlet on cognitive explanations for depression.
|
Assignment 7 - Section A questiona) Explain, in your own words, what is meant by a cognitive explanation of depression. [2]
(b) Describe a study investigating the cognitive explanation of abnormal affect. [4] |
Attribution theory and learned helplessness
Attribution theory suggests that when people experience something, they usually try and attribute a cause to that event. Some causes are within our control (e.g. our effort), and some are outside of our control (e.g. the weather).
The problem comes if we are continually attributing events to causes outside of our control. Pretty soon we will feel helpless, like nothing we do can make a difference to our situation. Seligman (1979) suggested that this learned helplessness was a key aspect of depression.
The problem comes if we are continually attributing events to causes outside of our control. Pretty soon we will feel helpless, like nothing we do can make a difference to our situation. Seligman (1979) suggested that this learned helplessness was a key aspect of depression.
Evaluating learned helplessness
|
Watch this 'Study.com' video, read the text and take the quiz to test your understanding of these ideas, and to learn about Seligman's famous research on dogs which he used to support the theory. 
Assignment 8 - Section A sample questiona) Explain, in your own words, what is meant by the term 'learned helplessness' (2)
b) Give one example of how learned helplessness might cause abnormal affect. (4) |
Bullet point 3 - Treatments for Depression
• treatments for depression
Biological: chemical/drugs (MAO, SSRIs); electro-convulsive therapy. Cognitive restructuring (Beck, 1979); rational emotive therapy (Ellis, 1962)
Biological: chemical/drugs (MAO, SSRIs); electro-convulsive therapy. Cognitive restructuring (Beck, 1979); rational emotive therapy (Ellis, 1962)
Biological treatments for depression - drug therapy
|
Exam Hint!!! Think like a psychologist and know the links!Although the actual drugs given to treat different psychological conditions vary; how they actually work and the evaluation issues around them have a lot of features in common. If you know them well, you can use the same issues in essays on ANY biological/drug treatments!
Before you read this section, look back at the way that drug therapy works (as described in the Schizophrenia section) and the issues associated with it. Then as you're going through this section, notice how you can apply the same issues here as well! |
|
You should remember from the above section on biological explanations, that the biochemical explanation for depression suggests that the condition is the result of low levels of serotonin and norepinephrine. If so, it follows that an effective drug therapy for depression
might involved using drugs that increase the supply of these
neurotransmitters. See the video to the right for an introduction to how this might happen.
Both serotonin and norepinephrine belong to a group of neurotransmitters called monoamines. Drug therapy is the most commonly used treatment for depression. Two of the most common drugs used are SSRIs and MAOIs. |
|
SSRIs (selective serotonin reuptake inhibitors)SSRIs are specific to serotonin. For example, fluoxetine (trade name Prozac) prevents the re-uptake of serotonin by the presynaptic neuron, so leaving it to have an enhanced effect on the postsynaptic neuron.
Usually used in bipolar depression rather than unipolar depression. |
|
MAOIs (monoamine oxidase inhibitors)Monoamine Oxidase (MAO) is an enzyme which normally breaks down monoamines at the synapse. MAOIs block MAO, thus the monoamines remain longer in the synapse and continue to act on the postsynaptic neuron.
|
Evaluating drug treatments for depression
You've seen these before!! A lot of them are the same as the issues with drug treatments for schizophrenia. They're the same as the issues for ALL drug treatments! |
|
Assignment 9 - Video analysisThe video to the right is a very nice, not too detailed look at some of the controversies surrounding the use of anti-depressant medication (and, by extension, many of the issues surrounding drug therapy as a whole).
Many of the key evaluation ideas that we have looked at already in the course are referred to (if not in name), such as:
Make a list of the major points raised in the discussion, and try to relate them to the topics we have already covered in Schizophrenia and Abnormal Affect. |
|
Electro-convulsive therapy (ECT)
ECT appears to be successful for cases of severe depression and acute mania. An electric current of between 70 and 130 volts is generally passed through the non-dominant brain hemisphere, and an anaesthetic and muscle relaxants are given before the treatment itself. 6 to 9 treatments may be given over a month or so.
|
|
|
Assignment 10 - Section C question
Complete the following question from memory - writing at least half a page.
a) Describe one biological treatment for abnormal affect (6)
a) Describe one biological treatment for abnormal affect (6)
Cognitive therapies for depression - Beck's Cognitive Restructuring
|
Remember Beck's cognitive triad for depression? Re-read the section above on this page if you don't.
Cognitive therapy believes that:
In recent years, there have been increasing efforts to add some of the more successful features of behavioural therapy to cognitive therapy. This combination is referred to as cognitive-behavioural therapy. CBTs will attempt to change or restructure BOTH the client’s cognitions AND their behaviours in combination. |
|
Beck (1976) argued that therapy for depression should involve uncovering and challenging and replacing the negative and unrealistic beliefs of depressed clients.
Beck’s therapy consists of challenging the negative cognitive triad (see earlier). There are four phases: 1. Increasing confidence and elevating mood 2. Challenging automatic negative thoughts 3. Identifying negative thoughts 4. Changing key attitudes and beliefs 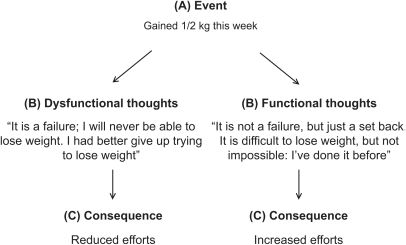
|
Clients examine the evidence on which their thougts are based, thus making them recognise they are faulty. The behavioural part then comes into play. Beck instructs his patients to monitor and log their thought processes between therapy sessions and gives them tasks that require patients to adopt new behaviours.
It is hoped that the client will come to accept that many of his or her negative thoughts are irrational and unrealistic. For example, a depressed client who argues that people are always avoiding him or her can be asked to keep a diary of specific occasions when it happens. It is very likely that it happens much less often than they imagine. |
Evaluating Beck's cognitive therapy
Research evidence - Hollon et al (2006)Aim – to compare the effectiveness of cognitive and drug therapy.
Method – People with moderate to severe depression were given either drug therapy or CBT for 16 weeks. Both groups were followed for a year. Results – CBT relapse rates were around 40%. Drug therapy rates were around 45%. A control group (on placebo) showed relapse rates of 80%. Conclusion – CBT appears to be as effective as drug therapy for treating depression. BUT… still a relapse rate of 40% or so, showing that using individual therapies on their own may not be the most effective form of treatment. Using an interaction of a number of different treatments may be the most effective form of treatment. |
|
|
Cognitive therapies for depression - Rational Emotive Therapy (RET), Ellis (1962)
|
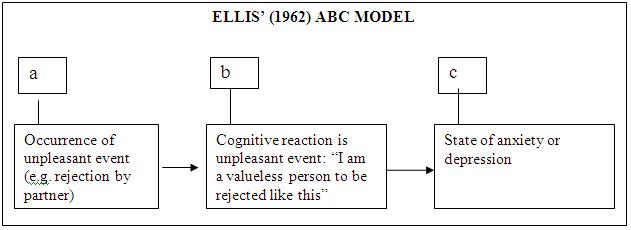
Albert Ellis (1962) was one of the first therapists to put forward a version of cognitive therapy. He argued that anxiety and depression occur as the end points in a three-point sequence (see right)
According to the A-B-C model, anxiety and depression do not occur as a direct result of unpleasant events. More precisely, these negative mood states are produced by the irrational thoughts that follow from the occurrence of unpleasant events. The interpretations that are produced at point B depend on the individual’s belief system. 
|
Ellis argued that individuals who are anxious or depressed should create a point D - this is a dispute belief system that slows them to interpret life’s events in ways that do not cause them emotional distress. What would an appropriate D point be for the example given above?
If this is done successfully, it will lead to an E - effective new emotional states. RET is in many respects very similar to Beck's therapy. Both involve attempting to replace faulty or irrational thoughts with more rational and effective ones. However, the 'dispute' section is unique to RET and means that it can be a more confrontational form of therapy than Cognitive Restructuring. The therapist is more in charge of interpreting the problem and offering a solution than in Beck's CBT. |
Assignment 10 - Practice your RET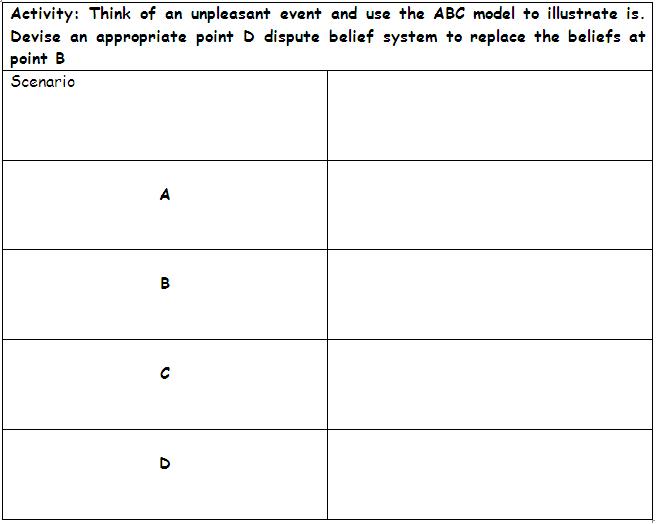
|
You can watch Albert Ellis perform a full RET session in this video. Try to identify the ABCD of the session. Note any interesting features and mention them in our next class discussion. |
Evaluating Rational Emotive Therapy
|
|
Other than these, all the evaluations of Beck's cognitive therapy ALSO APPLY TO ELLIS'! Both forms share many strengths and weaknesses, so make sure you know that you can use these evaluations for both.
Assignment 11 - Section C questionBeck (1967) outlined negative beliefs captured in the ‘cognitive triad’ as a cause of depression but also believed it could be treated.
(a) Describe the main features of cognitive behavioural therapy. [6] (b) Suggest how you would help a patient suffering from depression using cognitive behavioural therapy. [8] The cartoon on the right satirises the common consequence of thinking of depression as a cognitive disorder - that if it's all to do with thinking then the person should just be able to 'think' themselves better. Most of us probably still have a feeling that people with low mood should sometimes just 'pull themselves together' or 'cheer up'. Hopefully you now understand that this is not always as easy as it can seem.
|
|
End of section essay writing exercise - Section B
We'll now start looking at the Section B 'evaluate' question. The essay will have two parts, a 'describe' section and an 'evaluate' section.
14 a) Describe what psychologists have discovered about abnormal affect. [8]
14 b) Evaluate what psychologists have discovered about abnormal affect and include a discussion of competing treatments. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it 'competing treatments'. At least a paragraph should consequently be devoted to discussing and contrasting the different ways that depression can be treated.
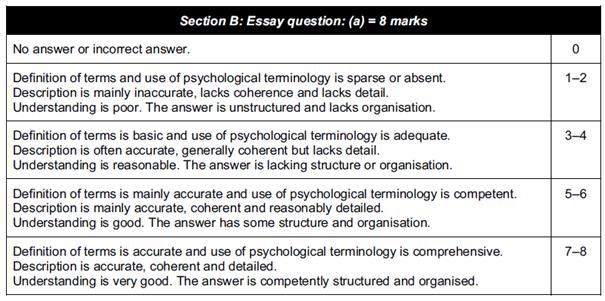
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.
14 a) Describe what psychologists have discovered about abnormal affect. [8]
14 b) Evaluate what psychologists have discovered about abnormal affect and include a discussion of competing treatments. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it 'competing treatments'. At least a paragraph should consequently be devoted to discussing and contrasting the different ways that depression can be treated.
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.

|

|
End of section essay writing exercise - Section C
Section C in your exam always consists of two questions, one 6 mark recall question and one 8 mark application question. There are always two of these types of question, and you need to choose one.
15 Ellis (1962) outlined Rational Emotive Therapy to treat depression, but he also believed it could help reduce stress.
(a) Describe the main features of rational emotive therapy. [6]
(b) Suggest how rational emotive therapy could be used to help students suffering from examination stress. [8]
16 Dr Phillips has two patients with depression. One, Kate, is a new patient who has never had depressive symptoms before but is finding coping very difficult indeed. The other patient, Sally, has been depressed for a long time and Dr Phillips has tried all kinds of different treatments without much success.
(a) Describe one suitable treatment for Kate. [6]
(b) Name one suitable treatment for Sally that is different from the one you described for Kate. Explain why this choice is more appropriate for Sally. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here in Q15 for example, you have to suggest how you would use REBT to treat the patient. You therefore need to make sure that you are specifically referring to ideas of REBT, and to the condition given in the question - stress. It takes some getting used to writing this way, but it is an area that, with a little bit of practice, you will be able to do very well on.
Have a go at the questions above. Please submit your essays through the form on the home page.
15 Ellis (1962) outlined Rational Emotive Therapy to treat depression, but he also believed it could help reduce stress.
(a) Describe the main features of rational emotive therapy. [6]
(b) Suggest how rational emotive therapy could be used to help students suffering from examination stress. [8]
16 Dr Phillips has two patients with depression. One, Kate, is a new patient who has never had depressive symptoms before but is finding coping very difficult indeed. The other patient, Sally, has been depressed for a long time and Dr Phillips has tried all kinds of different treatments without much success.
(a) Describe one suitable treatment for Kate. [6]
(b) Name one suitable treatment for Sally that is different from the one you described for Kate. Explain why this choice is more appropriate for Sally. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here in Q15 for example, you have to suggest how you would use REBT to treat the patient. You therefore need to make sure that you are specifically referring to ideas of REBT, and to the condition given in the question - stress. It takes some getting used to writing this way, but it is an area that, with a little bit of practice, you will be able to do very well on.
Have a go at the questions above. Please submit your essays through the form on the home page.
Revision |
ExtensionBelow is an interesting research article on the use of RET in treating women who have undergone genital mutilation.
The serotonin hypothesis for depression is not 50 years old. This very recent review gives an excellent (if complex) overview of its strengths and weaknesses, and the evidence which shows why it cannot be considered a full explanation of the condition.
| ||
