Anxiety Disorders (obsessions and compulsions)
Bullet point 1 - Definitions, measures and examples of obsessions and compulsions
• definitions, measures and examples of obsessions and compulsions
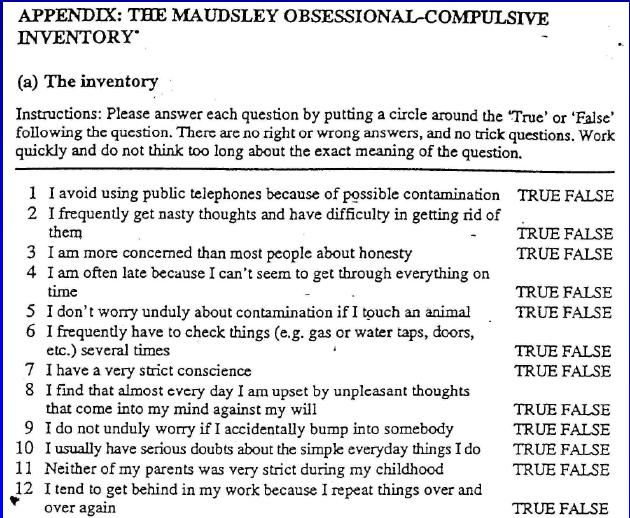
Defining obsessions and compulsions; case studies of/examples (e.g. ‘Charles’ by Rappaport, 1989); measures: e.g. Maudsley obsessive-compulsive inventory
Defining obsessions and compulsions; case studies of/examples (e.g. ‘Charles’ by Rappaport, 1989); measures: e.g. Maudsley obsessive-compulsive inventory
Defining OCD
|
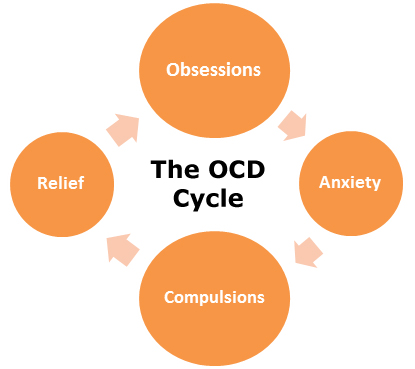
‘A disorder in which a person has recurrent and unwanted thoughts, a need to perform repetitive and rigid actions, or both’
This definition details both parts of the condition:
|
OCD and the DSMThe DSM-IV describes the main symptoms of OCD as:
• Recurrent obsessions and compulsions • Recognition by the individual that the obsessions and compulsions are excessive and/or unreasonable • That the person is distressed or impaired, and daily life is disrupted by the obsessions and compulsions. |
OCD occurs in approx 2% of the population and in men and women in equal numbers. The age of onset is usually adolescence or early adulthood, but is can also begin in childhood.
Common obsessive thoughts concern contamination, e.g. germs. The obsession occurs automatically and is unwanted and disturbing to the individual. The thoughts and images are not just normal anxieties, but excessive worries that are usually unrelated to real-life problems. What might a compulsion be for someone who has obsessive thoughts about germs?
If a person is prevented from performing the compulsion, feelings of dread and panic occur. People with obsessive-compulsive disorder also feel that they should resist the compulsion, but are unable to do so. Attempts are made to resist, but end in feelings of defeat and failure when the person gives in.
Common obsessive thoughts concern contamination, e.g. germs. The obsession occurs automatically and is unwanted and disturbing to the individual. The thoughts and images are not just normal anxieties, but excessive worries that are usually unrelated to real-life problems. What might a compulsion be for someone who has obsessive thoughts about germs?
If a person is prevented from performing the compulsion, feelings of dread and panic occur. People with obsessive-compulsive disorder also feel that they should resist the compulsion, but are unable to do so. Attempts are made to resist, but end in feelings of defeat and failure when the person gives in.
Case studies of OCDFor many sufferers of OCD their lives are so taken up with rituals that they are unable to function adequately or even hold down a job. For example, someone who feels compelled to keep washing may literally spend hours and hours in the shower and so not be able to get to work on time, or at all on some days. A person who is compelled to hoard and never throw anything away may find that after some years that the simply cannot move in their home because every room is full.
Charles was a boy who was unable to rid himself of a feeling of ‘stickiness’, despite 3 hours a day in the shower. His obsession was over the feeling of stickiness and his compulsive act was showering for hours. See the document below for more
Measuring OCD - The Maudsley obsessive-compulsive inventoryThe Maudsley obsessive-compulsive inventory (MOCI) was developed by Hodgson & Rachman (1977). It consists of a 30 item True/False self-report questionnaire. The scale assesses overt rituals and their related obsessions. The questions are divided into a series of four sub-scales including:
|
We ALL have some rituals and habits!Many of us have routines and rituals in our lives and performing them provides us with reassurance, however most people can adjust their lives if circumstances change their routine. When the routine or ritual becomes compulsive, repetitive and very time consuming it becomes a psychological disorder.
Kanner (1998) conducted research to find out the most common rituals and routines that people have: 
An individual obsessed with the thought of germ contamination might feel compelled to wash their hands up to 100 times a day, even sometimes scrubbing them with abrasive cleaners. The individual is aware that the rituals are unreasonable, yet feel compelled to perform them to ward off the anxiety associated with the obsessive thoughts of contamination.
Assignment 1 - Case studies of obsessions and compulsionsThe video below shows six youngsters with OCD. For each individual:
Finally, write an answer to the following question:
Evaluating the MOCI
Assignment 2 - Test your memory1. Describe one technique for measuring OCD (4)
2. Describe one case study of OCD (4) 3. a) Explain, in your own words, what is meant by the term ‘obsessive-compulsive disorder’. [2] (b) Using an example, describe what is meant by a compulsion. [4] | ||||
Bullet point 2 - Explanations of obsessive/compulsive disorder
• explanations of obsessive/compulsive disorder
Biomedical; cognitive-behavioural; psychodynamic
Biomedical; cognitive-behavioural; psychodynamic
Biomedical explanations for OCD
|
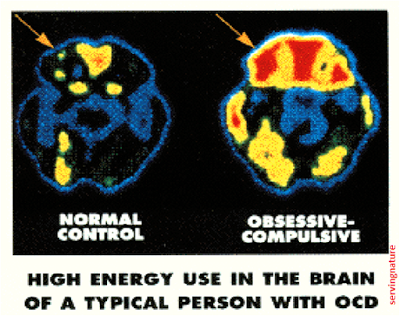
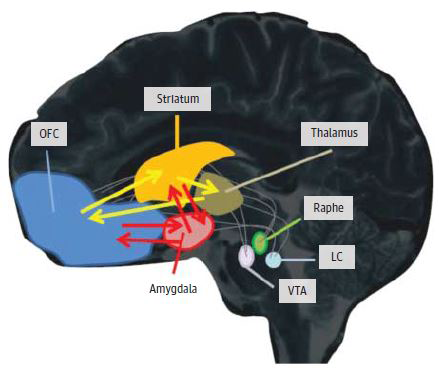
The biological approach suggests that OCD results from abnormal brain structure and/or functioning. The brain areas believed to be involved in OCD include the orbitofrontal cortex (OFC) and the thalamus.
The thalamus is a brain area whose functions include controlling checking and other safety behaviours. The OFC is involved in decision making and worry about social and other behaviour. In OCD the OFC and the thalamus are believed to be overactive. An overactive thalamus would result in an increased motivation to clean or check for safety. If the thalamus was overactive the OFC would also become overactive as a result. An overactive OFC would result in increased anxiety and increased planning to avoid anxiety. OCD symptoms are much more common in relatives of OCD patients, compared with the general population. What do these findings suggest about the causes of the brain abnormalities linked to OCD symptoms? |
|
Evaluating biomedical explanations for OCD
|
Research Evidence - Gilbert (2000)Decrease in thalamic volumes of pediatric patients with obsessive-compulsive disorder who are taking paroxetine (a type of SSRI). Gilbert et al (2000)
BACKGROUND:Thalamic dysfunction has been implicated in obsessive-compulsive disorder (OCD). While OCD frequently has its onset during childhood, to our knowledge, no prior study has measured neuroanatomical changes in the thalamus of patients with OCD near the onset of illness, and before and after treatment. METHODS:Volumetric magnetic resonance imaging studies were conducted in 21 psychotropic drug-naive children, aged 8 to 17 years, with OCD and 21 case-matched healthy comparison subjects. Magnetic resonance imaging studies were also conducted in 10 of the 21 patients with OCD after 12 weeks of monotherapy with the selective serotonin reuptake inhibitor, paroxetine hydrochloride. RESULTS:Thalamic volumes were significantly greater in treatment-naive patients with OCD than in controls but declined significantly after paroxetine monotherapy to levels comparable with those of controls. Decrease in thalamic volume in patients with OCD was associated with reduction in OCD symptom severity. CONCLUSIONS:Our findings provide new evidence of thalamic abnormalities in pediatric OCD and further suggest that paroxetine treatment may be paralleled by a reduction in thalamic volume. These reductions may, however, not be specific to paroxetine treatment and could be due to a more general treatment response, and/or spontaneous improvement in symptoms. Our findings are preliminary given the small sample size and our inability to measure discrete thalamic nuclei. Assignment 3 - Analysing research findingsRead the summary of Gilbert et al's (2000) research above. Then:
| ||
Cognitive-behavioural explanations for OCD
You should be able to guess a lot of this explanation already! You know how the cognitive approach works by this stage...
|
People who suffer from OCD have obsessive thoughts. When normal individuals have intrusive and obsessive thoughts they can usually dismiss them, but for people with OCD these thought cause great anxiety.
Cognitive theory proposes that people with OCD have a ‘cognitive bias’ when attending to environmental stimuli. For example, their attentional system might be hyervigilant (excessively careful and watchful). OCD sufferers memories may also be impaired, so they may not remember if they had switched the light off, for example. Williams et al 1997) argues that people with OCD have a cognitive vulnerability to anxiety and one way that this vulnerability is apparent is through hyper-vigilance when entering a new environment, for example:
Patients may try to suppress obsessive thoughts, which actually makes them more likely. This may lead to them performing their compulsion, which temporarily reduces anxiety but which makes the compulsion more likely to have to be repeated later. 
|

Hypervigilance is a symptom of irrational thinking
A case study of hypervigilance...Rachman (2004) outlines a case study of a patient with OCD that give a good account of hyper-vigilance.
A female patient has a severe fear of diseases, particularly the prospect of encountering other people’s blood. She had catastrophic thoughts about the probability of harm (e.g. contracting AIDS) coming from even a small plaster worn by someone. She over-estimated the seriousness of contact with anyone. When she went to a public place, she rapidly scanned the environment and the people she encountered, constantly on the lookout for evidence of blood, cuts, bandages etc. She tended to misperceive as blood a wide range of dark-coloured spots and her hypervigilant scanning meant that she could recall in great detail the blood-related items that she had encountered over many years. Assignment 4 - Section C Questiona) Describe the cognitive explanation of OCD (6)
Try to write half a page from memory
| ||
Evaluation of cognitive explanations for OCD
|
|
Psychodynamic explanations for OCD
|
The Freudian explanation of OCD is to do with conflict between the id, ego and superego (like always!)
The conflict is said to date back to early childhood, especially the anal and phallic stages of psychosexual development. Toilet training is one area where it has been suggested that children could develop unresolved conflicts, which can later develop into OCD On this model OCD is the result of trauma which has been repressed into the unconscious. The anxiety is manifested via the intrusive thoughts. The obsessional thoughts are the repressed memories of the trauma breaking through into consciousness, and the compulsive rituals are the conscious attempts to reduce anxiety caused by the thoughts. Evaluating the Psychodynamic explanation for OCDBEFORE YOU READ... WORK IT OUT!! It's the same answers each time...
|
Assignment 5 - recalling the psychosexual stagesWithout reading anything to the left:

|
Bullet point 3 - Treatments for obsessive/compulsive disorder
• treatments for obsessive/compulsive disorder
Drug therapy; cognitive-behaviour therapy; psychoanalytic therapy
Drug therapy; cognitive-behaviour therapy; psychoanalytic therapy
Drug therapy for OCD

As we have seen, researchers have learned that certain antidepressant drugs are very useful in the treatment of OCD. For example, the anti-depressant paroxetine was used by Gilbert et al (2000), who found improvements in their patients afterwards.
Paroxetine is an SSRI, leading to an increase in serotonin levels. You know how these drugs work from the Abnormal Affect page, so you should be able to describe the action of the drug in some detail. Not only do these SSRIs increase brain serotonin activity; they also produce more normal activity in the orbital region and caudate nuclei, the brain areas that are implicated in the disorder (Baxter et al., 2001).
Paroxetine is an SSRI, leading to an increase in serotonin levels. You know how these drugs work from the Abnormal Affect page, so you should be able to describe the action of the drug in some detail. Not only do these SSRIs increase brain serotonin activity; they also produce more normal activity in the orbital region and caudate nuclei, the brain areas that are implicated in the disorder (Baxter et al., 2001).
I could write more... but you don't need it!!
You got this! |
Evaluating drug therapies
|
Cognitive-behaviour therapy for OCD
 Classic catastrophic thinking...
Classic catastrophic thinking...
This therapy attempts to change the conscious thought processes. There are two initial steps involved.
Both approaches are done to help the person stop performing the compulsive behaviours. An additional techniques used in cognitive therapy is habituation training (Franklin et al 2000). Here the client is asked to think repeatedly about their obsessive thoughts. The idea is that by deliberately thinking about obsessions, they will become less anxiety raising, with the consequence that compulsive behaviour is not required to reduce high levels of anxiety.
Research has shown that cognitive therapy is successful in reducing the frequency with which people have obsessive thoughts. It has also seems to be effective in reducing both the frequency and the duration of compulsive behaviours (Rufer et al 2005).
For people who experience obsessions only, habituation training is often the entire plan of treatment (Rachman and Hodgson, 1989). For others, however, therapists may add covert – response prevention: they teach clients to prevent or distract themselves from carrying out compulsive actions that may occur during habituation training.
- Helping people to understand that they are misinterpreting their thoughts – misinterpretations include, thinking that the thought will become an actual behaviour, and feeling guilty and ashamed about having obsessive thoughts.
- Making people aware of how they try to neutralise the obsessive thoughts by attempting to make amends for having such thoughts.
Both approaches are done to help the person stop performing the compulsive behaviours. An additional techniques used in cognitive therapy is habituation training (Franklin et al 2000). Here the client is asked to think repeatedly about their obsessive thoughts. The idea is that by deliberately thinking about obsessions, they will become less anxiety raising, with the consequence that compulsive behaviour is not required to reduce high levels of anxiety.
Research has shown that cognitive therapy is successful in reducing the frequency with which people have obsessive thoughts. It has also seems to be effective in reducing both the frequency and the duration of compulsive behaviours (Rufer et al 2005).
For people who experience obsessions only, habituation training is often the entire plan of treatment (Rachman and Hodgson, 1989). For others, however, therapists may add covert – response prevention: they teach clients to prevent or distract themselves from carrying out compulsive actions that may occur during habituation training.
Exposure and response prevention (ERP)
 Exposed to something which would normally trigger the compulsion, patients are then prevented from performing their rituals...
Exposed to something which would normally trigger the compulsion, patients are then prevented from performing their rituals...
Cognitive treatment like those given above can often be paired with a more behavioural strategy such as ERP. ERP focuses only on the compulsions, whereas cognitive therapy tends to focus more on the obsessions (so together they are well matched). ERP deliberately exposes clients to objects or situations that cause anxiety and requires the client to resist performing the compulsive behaviour. The role of the therapist is to help the person develop ways in which they can resist performing the compulsive behaviours. A number of steps are usually involved:
ERP has been used in both one-to-one and group therapy sessions. Outside the therapy session, clients are asked to practise exposing themselves to feared situations and refraining from the compulsive behaviour.
Research which has followed by clients after ERP therapy has shown that between 55% and 75% show improvement and that the improvement lasts for 5 or 6 years (Franklin et al 2005).
- Informing the client about exposure and response prevention, and what the therapy will involve.
- Using what is called an exposure hierarchy, which starts with mildly anxiety-raising situations and goes through to the highest level of anxiety (similar to systematic desensitisation
- Repeated exposure to situations that cause high anxiety, until the level of anxiety reduces.
- Getting the client to resist and refrain from performing the compulsive behaviour.
ERP has been used in both one-to-one and group therapy sessions. Outside the therapy session, clients are asked to practise exposing themselves to feared situations and refraining from the compulsive behaviour.
Research which has followed by clients after ERP therapy has shown that between 55% and 75% show improvement and that the improvement lasts for 5 or 6 years (Franklin et al 2005).

|
Assignment 6 - strengths and weaknesses of cognitive treatmentsYou have already looked at the benefits and problems with cognitive therapies in detail throughout the 'Abnormality' course. You can show that understanding here:
Write a list of two or three positive and two or three negative evaluative comments about the treatments listed above. Use your general understanding of the cognitive approach, and apply relevant criticisms from other areas if you need to. This is great practice for an exam. Sometimes in an exam you won't know exactly what to say, but if you understand the general approach and use your common sense you will be able to come up with accurate evaluations of any approach. |
Psychoanalytic therapy for OCD
|
This treatment is similar to the treatment for phobias. The techniques of free association and dream analysis are used in an attempt to uncover the unconscious conflicts that have occurred during the anal and phallic stages of development. Psychodynamic therapy tries to get at the underlying cause of the disorder. It is assumed that the obsessive-compulsive symptoms will disappear once the conflicts have been brought to consciousness and analysed.
Traditional psychodynamic treatment of OCD would take between 2 and 5 years. These days, psychodynamic therapists offer much shorter therapy, over just a number of months. This therapy concentrates on helping the person take actions to lessen the impact of the disorder on daily life. Less attention is paid to the underlying causes buried in the unconscious and originating in early childhood. Assignment 7 - Analysing Rat Man
Read this translation of a section of Freud's manuscript about Rat Man.
How does this document illustrate Freud's theory in action? Write half a page answering this question. |
Case study - Rat ManThe rat man was a young lawyer who first saw Freud in October 1907. His real name was Ernst Lanzer. Ernst told Freud that he had disturbing thoughts about harm coming to his father and a young woman that he liked. The disturbing thoughts centred on a punishment he had been told about in the army. This punishment involved tying a pot of rats to a person’s buttocks and the rats entering the person through the anus. Ernst reported that
he thought about this happening to his father and the young lady. To ward off this image and thoughts that it might happen to his father, girlfriend and other people he was fond of, the Rat Man engaged in obsessive-compulsive rituals. Freud interpreted these thoughts and obsessive behaviours as resulting from the mixture of love and hate that he felt for his father. Unconsciously, Freud said, the Rat Man hated his father and wished to torture him with rats. Any thought of this would cause the Rat Nan to experience unbearable feelings of guilt and fear. The obsessive-compulsive behaviours helped to reduce the fear and feelings of guilt. Freud treated the Rat Man for about a year, after which he said that the treatment had ‘led to the complete restoration of the patient’s personality, and to the removal of his inhibitions’. In short, Freud claimed to have cured him of his phobia of rats and obsessive-compulsive tendencies. You don't even get told the evaluations of psychoanalytic treatments by now... you should know them already!
|
Evaluating treatments as a whole... weaving the threads together
It can seem daunting to learn all of the details of the different approaches for each different condition. There is a huge amount of information in this unit, so trying to learn it all is a real challenge. My tip is... DON'T! Here are two great ways of reducing the amount that you have to learn...
UNDERSTAND... don't just learnInstead of learning all these different areas off by heart, aim to UNDERSTAND how each approach works, and then APPLY this understanding to each condition.
If you already understand the pros and cons of the psychodynamic approach, for example it will be easy for you to see how these apply to the condition of OCD. YOU WON'T HAVE TO LEARN ANYTHING NEW! All you have to do is use your understanding to come up with the evaluation issues. |
Evaluate using other approachesDon't think that a piece of evidence for one approach is only useful for that approach... you can also use it when evaluating other explanations too!
For example, if you have a study which supports the cognitive explanation, THIS COULD ALSO BE USED AS EVIDENCE AGAINST THE BIOLOGICAL EXPLANATION. The same evidence can do more than one job, providing you write it clearly and use it to answer the question you have been asked. This means that you can use the same piece of evidence in two, or more, different points. Two for the price of one! |

If I had to sum all this advice up in one sentence it would be this:
Exam success (and good Psychology) does not happen by learning everything in little boxes and never making links across the syllabus; you need to LEARN LESS but to THINK MORE! |

|
End of section essay writing exercise - Section B
(a) Describe what psychologists have discovered about obsessive compulsive disorder. [8]
(b) Some psychologists argue that obsessive compulsive disorder is a result of suppressing disturbing thoughts into our subconscious. Evaluate what psychologists have discovered about obsessive compulsive disorder and include a discussion of the Psychodynamic explanation of obsessive compulsive disorder. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it the Psychodynamic explanation. At least a paragraph should consequently be devoted to discussing this.
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.
(b) Some psychologists argue that obsessive compulsive disorder is a result of suppressing disturbing thoughts into our subconscious. Evaluate what psychologists have discovered about obsessive compulsive disorder and include a discussion of the Psychodynamic explanation of obsessive compulsive disorder. [12]
First read this document, which covers the skills that we want you to learn when approaching these questions. In summary, you need to try to mention a range of information in question a), so try to mention things from all three bullet points in the specification (so here, something from each of the three approaches). For the question b), try to evaluate using issues and debates (same ones as from AS level). On this page, issues such as reductionism, determinism, ethics, data collection methods, scientific-ness, objectivity and other have been mentioned. Use these in your evaluations! Remember to use a PEE format if you find it helpful.
One final point. Make sure you answer the specific question asked! The 2 b) question will always have a little extra requirement in it, where it will ask you to focus your discussion on one specific area or issue. Here is it the Psychodynamic explanation. At least a paragraph should consequently be devoted to discussing this.
Generic mark schemes are given below. Read them carefully before you start writing and make sure your essays fulfill all the requirements. Please submit your essays through the form on the home page.


|

|
End of section essay writing exercise - Section C
Section C in your exam always consists of two questions, one 6 mark recall question and one 8 mark application question. There are always two of these types of question, and you need to choose one.
If obsessive compulsive disorder is caused by chemical imbalances in the brain then restoring balance should eliminate any symptoms of obsessive compulsive disorder.
(a) Describe the biological explanation of obsessive compulsive disorder. [6]
(b) Suggest what drug therapy could be used to help patients suffering from obsessive compulsive disorder. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here you have to suggest how you would use drugs to treat a patient with OCD. You therefore need to make sure that you are specifically referring to drugs and practices of drug therapy, and justifying your design using real life evidence and examples.
Have a go at the questions above. Please submit your essays through the form on the home page.
If obsessive compulsive disorder is caused by chemical imbalances in the brain then restoring balance should eliminate any symptoms of obsessive compulsive disorder.
(a) Describe the biological explanation of obsessive compulsive disorder. [6]
(b) Suggest what drug therapy could be used to help patients suffering from obsessive compulsive disorder. [8]
The first question is a straightforward recall question. This is the longest question you will get which could focus on just a single theory. You need to write about half a page, so a simple revision check is to make sure that you can write half a page of description about every idea/theory/study that is specifically mentioned in the specification.
The second question allows you to be creative. There is no single right answer. All you have to do is give practical and specific ideas for how you might implement the theory you have described in the first question into the scenario they give you. About a page should be a good length.
Here you have to suggest how you would use drugs to treat a patient with OCD. You therefore need to make sure that you are specifically referring to drugs and practices of drug therapy, and justifying your design using real life evidence and examples.
Have a go at the questions above. Please submit your essays through the form on the home page.
Revision |
Extension |
